


There is growing concern regarding the contribution of infilled turf fields on increased athlete infections. Abrasions that occur on these fields create a port of entry for pathogens such as Staphylococcus aureus that are present on the athlete’s skin or possibly on the field’s surface. This study compares the occurrence of microbial populations on two infilled synthetic turf fields (year old turf vs. 6 year old turf) in three locations. Both fields were sampled once a week for at least 14 weeks (exact number varied on field and location) during the late summer and fall of a football season. Sites sampled included the sidelines, the middle of each field, and the end of each field. Tryptic Soy Agar was used to determine total microbial load, Mannitol Salt Agar for Staphylococcus, and Eosin Methylene Blue Agar to count the number of enteric organisms such as Escherichia coli. Much higher microbial populations were found on the older turf field with as much as a 104 increase over similar locations on the newer turf. This suggests microbial populations can accumulate in synthetic turf infill from year to year.
When comparing the bacterial load on different areas of the field, the sideline had the highest counts with an average of 1.12×108 CFUs (colony forming units) per gram of rubber infill on the older field. On the new synthetic turf, the area with the highest number of total microorganisms was also the sideline, with an average of 2.5×105 CFUs per gram of infill. A high number of salt-tolerant bacteria were able to grow on MSA, indicating possible staphylococci, with an average of 2.77×102 CFUs per gram on the new field and 6.58×103 CFUs per gram on the older field. These results indicate that infill material can serve as a source for the spread of pathogens among student athletes, and that these organisms seem to accumulate over time posing a greater risk if proper turf cleaning is not regularly performed.
Introduction
There is growing concern regarding the contribution of infilled turf fields to athlete infections. The overall spread of Staphylococcus, respiratory infections, and enteric infections have steadily increased over time, including in athletic settings (Cohen, 2005; Kirkland and Adams, 2008). Sport related skin infections have gained national attention and generated public interest, with many athletes and teams reporting increased incidents of skin and soft tissue infections (Cohen, 2008; Kazakova et al., 2005; Nguyen et al., 2005). These findings have provided impetus for more research to be done on the source of such infections particularly in athletic settings. It is known that athletes participating in contact sports have a higher risk of acquiring methicillin-resistant Staphylococcus aureus (MRSA) and other pathogenic bacteria, and football players have been shown to carry S. aureus more frequently than control groups (Oller et al., 2010). One important risk factor that may lead to increased infections for football players is the large number of abrasions they receive while practicing and playing on synthetic turf fields.
Vidair (2010) showed that the rate of skin abrasions due to contact with the turf was two- to three-fold higher for college soccer players competing on synthetic turf compared to natural turf. While the seriousness of individual skin abrasions was similar on the two surfaces, the higher skin abrasion rate increases the risk of skin infections in athletes using synthetic turf relative to natural turf (Vidair, 2010). These injuries, even if they appear insignificant, create a portal of entry for pathogens such as S. aureus (Begier et al., 2004).
Synthetic turf is being used in more applications than ever before. One of the great appeals of synthetic turf is the simple fact that it never needs to be fertilized, mowed or watered. Maintenance isn’t completely eliminated, but it is much simpler, less expensive and less labor intensive. This allows universities and other recreational facilities to save resources and increase revenue since they are decreasing maintenance costs. When Ohio State University announced the decision to go with synthetic turf, they noted the primary reasons were increased
practice and play frequency, the synthetic turf field’s playability in various weather conditions, and the consistency of the artificial surface (York, 2012). While skin and soft tissue infections are spread in a variety of ways, this study focused on the microbial populations found within synthetic turf fields as a potential source of pathogens when skin abrasions serve as a portal of entry. With a new synthetic turf field being installed the previous year, the opportunity presented itself to compare the microbial populations between the new turf field and a six-year-old synthetic turf field on the same university campus in Ogden, Utah. More specifically, we investigated whether there were any differences in microbial populations between two separate synthetic turf fields in similar time periods and locations. This study provides insight into: existence of harmful bacteria on synthetic turf fields, the amount and kind of bacteria present on each field, the specific areas on turf fields in which they exist, and whether increased use of turf fields affects these microbial populations. Application of these findings could impact the frequency of cleaning of the infilled turf field to help prevent infection, and provide a better understanding of the risks that athletes face when playing on synthetic turf fields.
Materials and Methods
Synthetic Turf Field Sampling
Two infilled turf fields were sampled, a new synthetic turf field completed one year before this study and an older one, installed six years prior (Table 1).
The rubber infill crumb was sampled from three locations on each field every one to two weeks for 4 months throughout the late summer and fall of the 2012 football season with microbial enumeration done on three selective media. Sites sampled included the sideline (near the 50 yard line), the middle of the field, and the end of the field (Figure 1). These sites were sampled on both fields. Games are held on the new field, and both fields are used for practice primarily by the football team at Weber State University in Ogden, Utah. The two fields are located only 0.7 miles apart.
Microbiological Enumeration
Rubber infill was collected from each test site by using a sterile spatula to scoop infill material into a sterile Whirlpak bag. Ten grams of rubber infill was stomached in 90 ml of sterile phosphate buffer for four min at 260 rpm using a Stomacher 400 Circulator (Seward Laboratory Systems Inc., Bohema, NY).
Tryptic Soy Agar (TSA) (Hardy Diagnostics, Santa Maria, CA) was used to determine total microbial load, Mannitol Salt Agar (MSA) (Becton, Dickinson, and Co., Sparks, MD) for S. aureus, and Eosin Methylene Blue Agar (EMB) (Hardy Diagnostics, Santa Maria, CA) to determine the number of coliforms such as Escherichia coli. After serial tenfold dilutions using sterile phosphate buffer as the diluent were done, spread plates were done an each media to enumerate samples. Samples of the old turf infill were plated on TSA at dilutions up to 10-6 for the sideline and up to 10-5 for the center and end of the field. Samples of the new turf infill were plated on TSA up to the 10-4 dilution. Samples of the old turf infill were plated on EMB at dilutions up to 10-2, while only the 10-1 dilution was used for the new turf infill. Samples from both fields were plated on MSA at a dilution of 10-1 for all locations. These dilution ranges were selected to fit the countable ranges of each location on each field after the first plating trial. All inoculated plates were incubated at 37oC for 48 hours and then CFUs were enumerated. EMB plates were incubated in gaspaks.
Confirmation of S. aureus Isolates
Potential S. aureus colonies found on the MSA plates were aseptically picked off and quadrant steak plated for the single colony isolation.
Staphylococcus aureus was confirmed by the indication of mannitol fermentation on MSA, a positive coagulase test (Coagulase Plasma, Rabbit with EDTA; Becton, Dickinson, and Co., Sparks, MD) performed on a slide, and the observation of Gram-positive cocci using the Gram stain.
Statistical Analysis
A comparison was done between the two fields at each site to determine differences between microbial loads. Means at each site were determined and compared both for each sample time and over the test period. In order to obtain T test data, GraphPad software was used at the website: http://www.graphpad.com/quickcalcs/ttest1.cfm. A paired T test was performed using all of the collected microbial counts at each location. The old and new turf fields were compared by microbial load for each media in each location.
Results and Discussion
Total Microbial Loads: Old vs. New Turf
Higher microbial populations were found on the older turf field (as much as a 104 increase over similar locations on the new turf), as well as in areas of high traffic such as the sidelines. This suggests microbial populations can accumulate in synthetic turf infill from year to year. When comparing the microbial load on different areas of the field, the sideline on the older turf had the highest bacterial counts with an average of 1.12 x 108 CFUs per gram of rubber infill on the older turf (Figure 3). On the new turf, the area with the highest number of total microorganisms was also the sideline, with an average of 2.50 x 105 CFUs per gram of infill (Figure 3). A paired T test showed the differences between old and new turf total bacterial loads in each location were significant (Table 2). These bacterial counts are comparable to results by McNitt et al. (2008) who found up to
8.0 x 104 per gram of infill and Vidair (2010) with infill bacterial loads as high as 5.3 x 104 CFU per gram. Both studies used much smaller sample sizes for analysis and agitated samples for a considerably shorter time period prior to dilution which may have led to lower bacterial counts.
Bacterial Loads using MSA and EMB
Counts from the MSA plates revealed a relatively high number of mannitol-fermenting salt-tolerant bacteria, a possible indication of staphylococci, with an average of 2.77 x 102 CFUs per gram of infill on the new turf and 6.85 x 103 CFUs per gram of infill on the older turf (Figure 4). The sideline was the only location that showed a significant difference between old and new turf when plating on MSA (Table 2). McNitt et al. (2008) failed to isolate S. aureus from any samples of infill while Vidair (2010) found presumptive Staphylococcus species in the infill from 2 of 30 synthetic fields samples but did not speciate further nor confirm the initial isolations.
A similar trend was noted when infill samples were plated on EMB agar from the two fields. Enteric bacterial counts were higher on the old turf than on the corresponding position of the new turf field (Figure 5). Similar to bacterial loads on MSA, the sideline was the only location to show a significant difference between old and new turf when the infill was plated on EMB (Table 2). Of note, E. coli was isolated using EMB agar on the newer turf as indicated by colony appearance on the EMB agar, in an area of high usage, the sideline.
Conclusions
These results indicate that infill material can serve as a potential source for the spread of bacterial pathogens among athletes and that these organisms seem to accumulate over time posing a greater exposure risk if proper cleaning is not routinely performed. Specifically, areas with increased human traffic especially the sidelines on both the old and new synthetic turf fields had increased microbial loads when compared to less frequently used areas of the fields. During the fall football season, many of the athletes, coaches and athletic staff are stationed on the sidelines. This leads us to believe that increased human traffic results in a higher microbial count, perhaps due to spitting, sweating, bleeding, drink water, sport drinks, etc. In addition, S. aureus was initially indicated to be present in situ on one of the synthetic turf fields, which is in contrast to an other study where they could not find this pathogen on their synthetic turf samples (Serentis, McNitt and Petrunak, 2011). This difference may be due to the use of a different selective media since Serentis et al. (2011) used Baird Parker Agar while we used of MSA or even the amount of infill turf sampled. Serentis et al. (2011) sampled only 0.075 grams of infill versus our study, which sampled 10 grams of infill each time. Another difference was their turf samples were collected in the summer while our samples were collected in the fall and early winter when field temperatures were lower and thus more conducive to survival of S. aureus. These observations also hold true for comparisons with the studies of synthetic turf done by McNitt et al. (2008) and Vidair (2010), both of which could not confirm S. aureus in their infill samples. In addition to the artificial turf microbial results, these athletes are certainly at risk while training indoors as noted by the presence of MRSA on shared athletic equipment (data not shown). All of these data underscores the fact that collegiate athletes are at risk both on and off the field for exposure to potential pathogens.
This knowledge of the microbial load at specific sites on each turf field and their accumulation over time should assist with providing useful interventions by athletic trainers and other medical staff. As athletic medical personnel endeavor to prevent infections, as well as help athletes heal in the quickest time possible, it would aid their cause to know where bacteria counts are highest so that they can provide each athlete with the safest environment possible (Kahanov, 2011). The limited scope of this current study and the paucity of studies by others on this topic illustrate the need for further research to ameliorate this expanding problem.
References
Begier, E.M., K. Frenette, N. L. Barrett, P. Mshar, S. Petit, D. J. Boxrud, K. Watkins-Colwell, S. Wheeler, E. A. Cebelinski, A. Glennen, D. Nguyen, and J. L. Hadler. (2004). A high-morbidity outbreak of methicillin-resistant Staphylococcus aureus among players on a college football team, facilitated by cosmetic body shaving and turf burns. Clinical Infectious Diseases 39: 1446-53.
Cohen, P.R. (2005). Cutaneous community-acquired methicillin-resistant Staphylococcus aureus infection in participants of athletic activities. South Med J. 2005; 98(6): 596-602.
Cohen, P.R. (2008). The skin in the gym: a comprehensive review of cutaneous manifestations of community-acquired methicillin-resistant Staphylococcus aureus infection in athletes. Clinics in Dermatology 26:16-26.
Kahanov, L., E. J. Gilmore, L. E. Eberman, J. Roberts, T. Semerjian, and L. Baldwin. (2011). Certified athletic trainers’ knowledge of methicillin-resistant Staphylococcus aureus and common disinfectants. Journal of Athletic Training 46(4):415-423.
Kazakova, S. V., J. C. Hageman, M. Matava, A. Srinivasan, L. Phelan, B. Garfinkel, T. Boo, S. McAllister, J. Anderson, B. Jensen, D. Dodson, D. Lonsway, L. K. McDougal, M. Arduino, V. J. Fraser, G. Killgore, F. C. Tenover,
S. Cody, and D. B. Jernigan. (2005). A clone of methicillin-resisant Staphylococcus aureus among professional football players. NEJM 325 (5):468- 75.
Kirkland, E.B. and B. B. Adams. (2008). Methicillin-resistant Staphylococcus aureus and athletes. J Am Acad Dermatol 59: 494-502.
McNitt, A.S., D. Petrunak, D. and T. Serensits, T. (2008). A survey of microbial populations in infilled synthetic turf fields. Pennsylvania State University, Department of Crop and Soil Sciences, available at http://www.fieldturf.com/images/downloads/penn-state-university-staph- study.pdf
Nguyen,D. M., L. Mascola, and B. Bancroft. (2005). Recurring methicillin- resistant Staphylococcus aureus infections in a football team. Emerging Infectious Diseases 11(4): 526-532.
Oller, A. R., L. Province, and B. Culress. (2010). Staphylococcus aureus recovery from environmental and human locations in 2 collegiate athletic teams. J Athletic Training 45:222-229.
Serentis,T. J., A. S. McNitt, and D. M. Petrunak. (2011) Human health issues on synthetic turf in the USA. Proceedings of the Institute of Mechanical Engineers, Part P, Journal of Sports Engineering and Technology 225(3): 139-146.
Vidair, C. (2010). Safety Study of Artificial Turf Containing Crumb Rubber Infill Made From Recycled Tires: Measurements of Chemicals and Particulates in the Air, Bacteria in the Turf, and Skin Abrasions Caused by Contact with the Surface. California Department of Resources Recycling and Recovery. Publication # DRRR-2010-009.
York, T. (2012). Beyond the Basics: Synthetic Turf Fields Have Come a Long Way. Recreation Management Magazine.

Figure. 1. Sample locations on new turf field (end, sideline, center). Sample locations are comparable on old turf field.
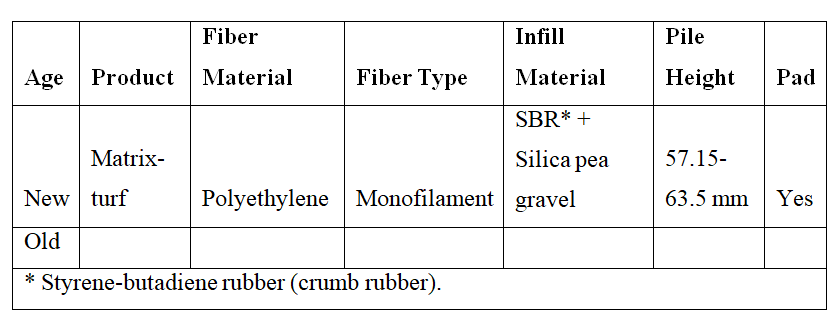
Table 1. Characterization of the two synthetic turf systems.
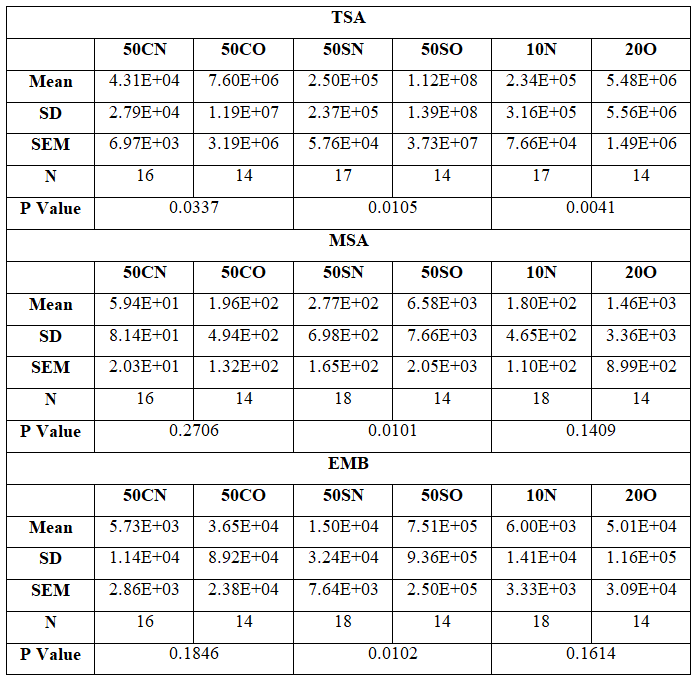
Table 2. Paired T test showing a significant increase in bacterial load based on similar locations. A significant increase was seen on all locations when using TSA. A significant increase was only seen on the sideline when using MSA and EMB. Numbers represent the yard line on the field, C represents center, S represents sideline, and N and O represent new and old, respectively.
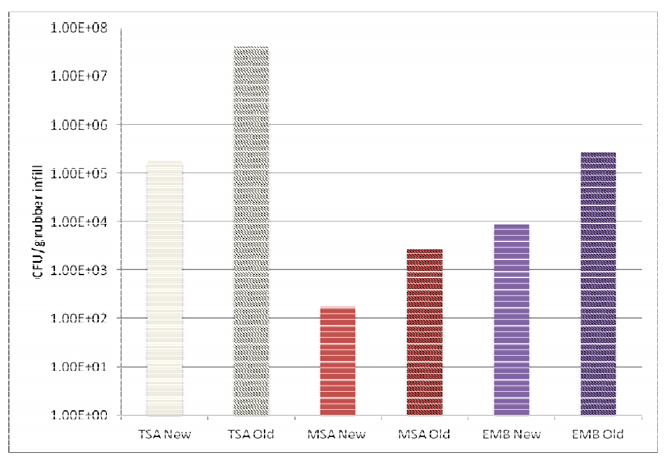
Figure 2. Comparison of overall averages (combining all three test locations) for the three media: New vs Old Turf. Error Bars were not used because an overall average of each medium was plotted.
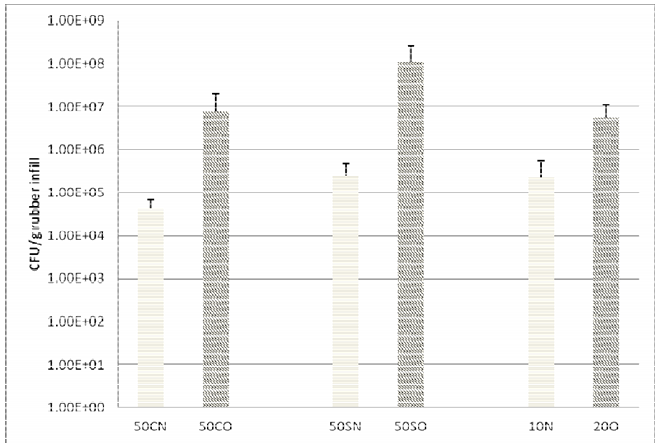
Figure 3. Total plate counts (TSA): New vs Old Turf. Numbers represent the yard line on the field, C represents center, S represents sideline, and N and O represent new and old, respectively.
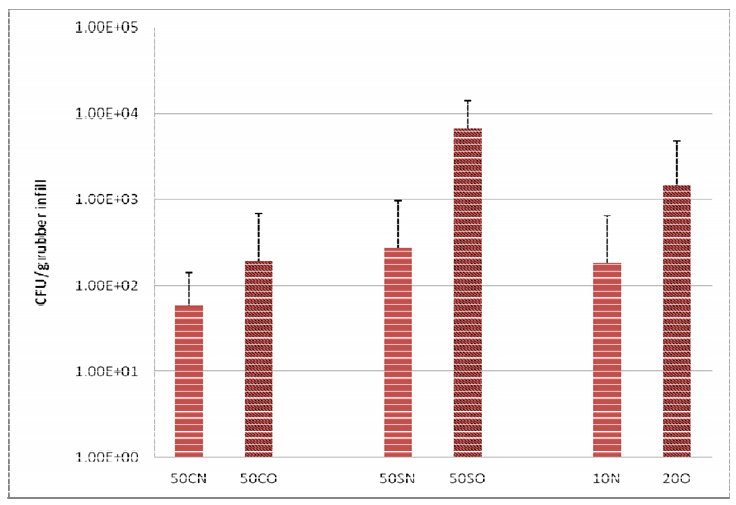
Figure 4. Staphylococcal counts (MSA): New vs Old Turf. Numbers represent the yard line on the field, C represents center, S represents sideline, and N and O represent new and old, respectively.
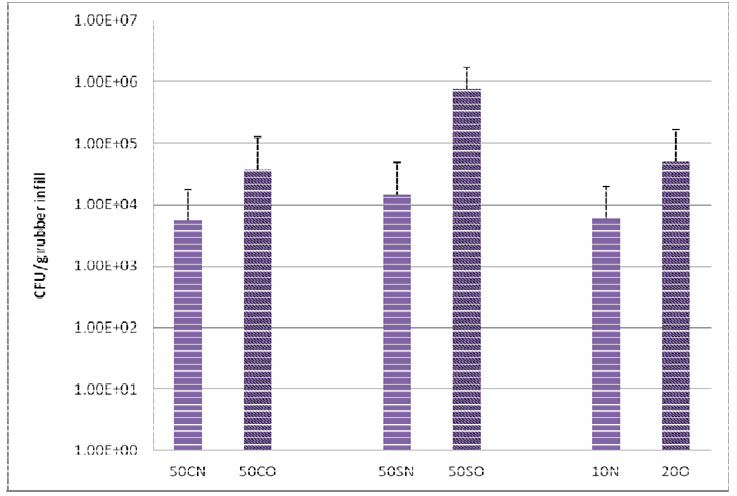
Figure 5. Enteric bacteria counts (EMB): New vs Old Turf. Numbers represent the yard line on the field, C represents center, S represents sideline, and N and O represent new and old, respectively.
0 Comments